
Understanding ACDF Surgery
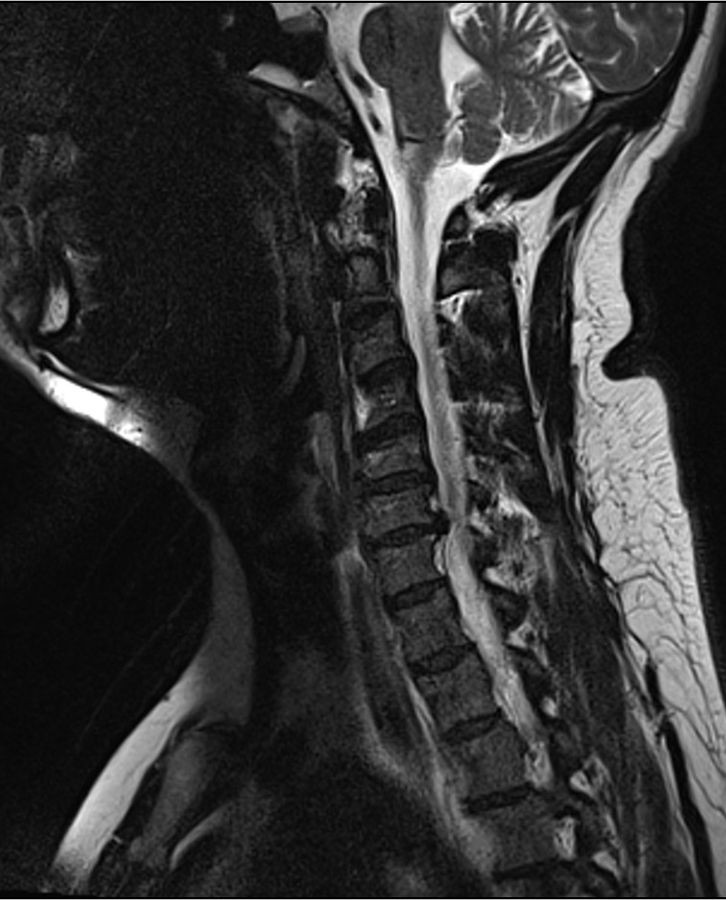
Anterior Cervical Discectomy and Fusion (ACDF) is a common surgical procedure used to treat nerve compression (radiculopathy) or spinal cord compression (myelopathy) in the neck (cervical spine). The surgery involves removing a damaged or herniated disc that is pressing on a nerve or the spinal cord, followed by fusing the adjacent vertebrae together to stabilize the spine.
Why is ACDF Recommended?
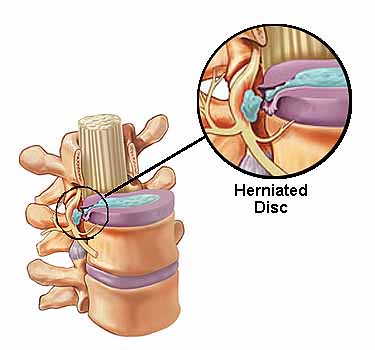
- Herniated or Degenerated Discs: When a disc bulges or ruptures, it can compress nerves, causing pain, numbness, or weakness in the arms or hands.
- Bone Spurs (Osteophytes): Arthritis can lead to bony overgrowths that narrow the spinal canal (spinal stenosis) or nerve openings (foraminal stenosis).
- Cervical Radiculopathy: Pinched nerves causing shooting pain, tingling, or muscle weakness.
- Cervical Myelopathy: Spinal cord compression leading to balance issues, clumsiness, or loss of fine motor skills.
Step-by-Step Surgical Process
1. Anesthesia
General anesthesia is used, so you will be asleep during the procedure.
2. Incision
A 3-5 cm horizontal cut is made on the front of the neck, usually along a natural skin crease.
3. Disc Removal
The surgeon carefully moves aside muscles and organs to reach the spine and removes the damaged disc.
4. Fusion
A bone graft or synthetic spacer is placed in the empty disc space, often secured with plates and screws.
5. Closure
The incision is closed with sutures or surgical glue.
Comprehensive Recovery Timeline
Hospital Stay
(1-2 Days)
- You may have a drain tube to remove excess fluids
- Pain is managed with medications
- Encouraged to walk the same day or next morning
- Possible temporary sore throat or swallowing discomfort
At-Home Recovery
(First Six Weeks)
- Neck Brace: A soft or hard collar may be recommended for support
- No heavy lifting (more than 5-10 kg)
- Avoid bending or twisting the neck
- No driving for 6 weeks
- Typically booked off work for full six weeks
Long-Term Healing
(3-12 Months)
- The bone graft gradually fuses the vertebrae (solid fusion takes ~3-6 months)
- Physical therapy may be recommended
- Follow-up X-rays or CT scans will check fusion progress
- Gradual return to all normal activities
Potential Risks and Complications
- Infection: At the incision site or deeper in the spine
- Nerve Injury: May cause temporary or permanent numbness/weakness
- Difficulty Swallowing (Dysphagia): Usually temporary due to swelling
- Hoarse Voice: If the vocal nerve is irritated
- Failed Fusion (Pseudarthrosis): The bones don't fuse properly
- Adjacent Segment Disease: Increased stress on nearby discs over time
Activity Guidelines After Surgery
First Six Weeks:
- Wear neck brace as directed (usually 1-6 weeks)
- No heavy lifting (more than 5-10 kg)
- Avoid bending or twisting the neck
- No driving - requires excessive neck use
- Gradual return to light activities
Long-Term Considerations:
- Maintain good neck posture
- Physical therapy to restore strength and flexibility
- Avoid smoking (impairs healing)
- Periodic follow-up imaging as recommended
When to Seek Immediate Care
Contact your surgical team immediately if you experience:
- Severe neck pain or swelling that worsens
- Fever/chills (sign of infection)
- Difficulty breathing or swallowing (unrelated to normal post-op swelling)
- New numbness, weakness, or loss of bladder/bowel control
Long-Term Outlook
ACDF surgery offers excellent outcomes for properly selected patients:
- Most patients experience significant pain relief and improved function
- Full recovery can take up to 12 months, depending on fusion success
- Maintaining good posture and neck exercises can improve healing
- Follow-up care is important to monitor fusion progress